Stay Current:
Pediatric Surgery—there's an app for that!
Find a customizable feed of newly released articles from the leading pediatric surgery journals right at your fingertips. Explore the articles our editors and your colleagues are talking about. Discover podcasts with expert discussions on hot topics in the field. Search our vast multimedia library to find articles, reviews, lectures, technique videos, infographics, guidelines, and podcasts. CME credit is available for select content. Presented by Cincinnati Children's Hospital and Children's Mercy Hospital, in partnership with Journal of Pediatric Surgery.
Available on the AppStore Get it on Google PlayWelcome!
Back to Guidelines
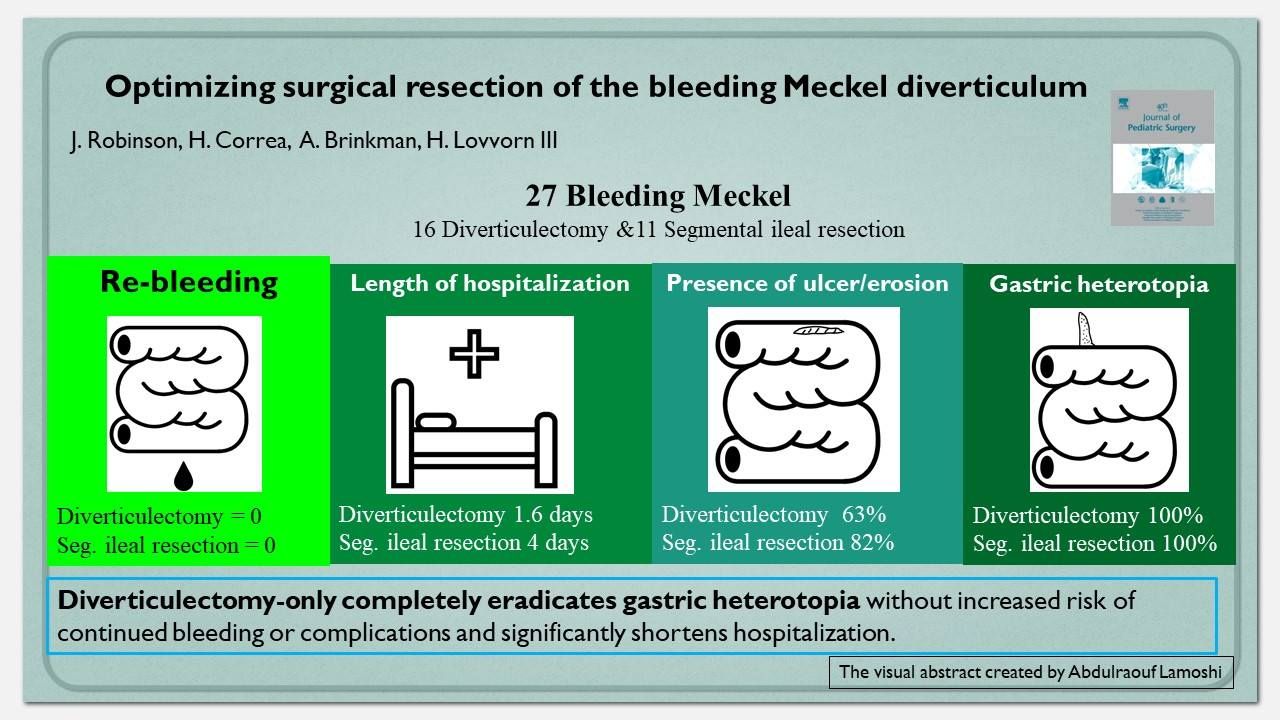
Optimizing surgical resection of the bleeding Meckel diverticulum in children
Purpose
Meckel diverticula containing gastric heterotopia predispose to local hyperacidity, mucosal ulceration, and gastrointestinal bleeding in children. Eradication of acid-producing oxyntic cells is performed by either of two surgical methods: segmental enterectomy including the diverticulum or diverticulectomy only.
Methods
Retrospective review of all children having surgical resection of a Meckel diverticulum at a tertiary-referral children's hospital from 2002 to 2016 was performed. Demographic data, surgical method, pathological specimens, and outcomes were evaluated.
Results
102 children underwent surgical resection of a Meckel diverticulum during the study period. 27 (26.5%) children presented with bleeding, of which 16 (59%) had diverticulectomy only, and 11 (41%) had segmental ileal resection. All Meckel diverticula in children presenting with bleeding contained gastric heterotopia, and resection margins were free of gastric mucosa. Histologically, 19 specimens showed microscopic features of ulceration, on average 2.95 mm (SD 4.49) from the nearest gastric mucosa (range: 0–16 mm). Mean length of hospitalization after ileal resection was 4.0 days (SD 1.2) compared to 1.6 days (SD 0.9) for diverticulectomy only (p < 0.001), with no re-bleeding occurrences.
Conclusion
In the operative management of children having a bleeding Meckel diverticulum, diverticulectomy-only completely eradicates gastric heterotopia without increased risk of continued bleeding or complications and significantly shortens hospitalization.
Level of evidence
Treatment Study: Level III.